Mirga Gražinytė-Tyla, who was Principal Conductor at Konzert Theater Bern from 2013 to 2015, has been appointed Associate Artist with the City of Birmingham Symphony Orchestra (CBSO).
PM/SMZ/wb
(translation: AI)
- Nov 15, 2023
Mirga Gražinytė-Tyla (Image: CBSO/Hannah Fathers)
Gražinytė-Tyla, who trained with Johannes Schläfli at the Zurich University of the Arts, among others, is currently Principal Guest Conductor with the CBSO and was the ensemble's Music Director from 2016 to 2022. In her new position, she will return to Birmingham regularly to continue her collaboration with the orchestra and choirs.
Founded in 1920, the City of Birmingham Symphony Orchestra is one of the most important orchestras in England, alongside the major London orchestras. Its last chief conductors were Simon Rattle (1980-1998), Sakari Oramo and Andris Nelsons (2008-2015) as Gražinytė-Tyla's predecessor. It is currently conducted by Kazuki Yamada (since 2023).
Ivanova winner of the Concours de Genève 2023
Elizaveta Ivanova, a student of Felix Renggli's flute class in Basel, is the winner of the Concours de Genève 2023 in the flute category.
PM/SMZ/wb
(translation: AI)
- Nov 10, 2023
Elizaveta Ivanova (Image: CdG Youtube video still)
Elizaveta Ivanova grew up in St. Petersburg, where she studied at the State Conservatory with Olga Chernyadeva. She then continued her studies with Felix Renggli at the Hochschule für Musik in Basel, where she graduated with a Master's degree in Special Performances in summer 2023. She has already excelled in numerous international competitions (Cluj, Crusell, Larrieu) and is a co-soloist in the Frankfurt Opera Orchestra, where she also lives.
The Concours de Genève offers a comprehensive career development program that provides support and advice to promote careers. In addition to the official prizes, the prizewinners benefit from two years of management by the concert agency Sartory Artists. The key to a series of performances that will enable them to take their first steps in Swiss and international concert halls.
Suisseculture concerned about the Federal Council's position
Suisseculture welcomes the Federal Council's rejection of the so-called halving initiative, but criticizes the fact that it wants to reduce the levies for radio and television by means of an ordinance.
PM/SMZ/wb
(translation: AI)
- Nov 09, 2023
(Image: SRG)
In its press release, the umbrella organization of cultural professionals in Switzerland recalls that the Swiss voted against the No Billag initiative five years ago by 71.6 percent. The Federal Council's plan to reduce the fees for radio and television by ordinance and partially release the industry from the obligation to pay contributions "does not take into account the support of the population and damages the public service mandate of SRG SSR instead of supporting it".
Instead of talking about the performance and impact of the SRG, Suisseculture continues, the initiative only talks about financing. At the media conference, Federal Councillor Rösti himself stated that it would not make sense to stipulate the amount of the radio and television levy in the Federal Constitution, as the initiative demands. This approach is at odds with the current world situation, in which information manipulated by artificial intelligence is creating even more uncertainty.
"Beethoven's Workshop" at the Academy of Sciences and Literature in Mainz combines genetic text criticism and digital music editing. Johannes Kepper is tackling the project at Paderborn University.
PM/SMZ/wb
(translation: AI)
- Nov 08, 2023
(Image: Videostill beethovens-werkstatt.de)
Genetic textual criticism is dedicated to compositional writing processes, which can be observed and approximately reconstructed both in individual autographs and in the sequence of interrelated workshop manuscripts (sketches, working manuscripts, lists of corrections, etc.). Writing processes provide information about Beethoven's compositional thinking, actions and decisions. Source documents and text-genetic results will be presented digitally as part of the project.
The musicologist Johannes Kepper has now taken up his academy professorship (W2) in the field of digital music editing and digital humanities. The professorship complements the Department of Musicology/Digital Music Edition at the Detmold/Paderborn Musicology Seminar of the Faculty of Cultural Studies at Paderborn University. In addition to his involvement in the academy project Beethoven's Workshop, Kepper will support the expansion of the "Center Music - Edition - Media" (ZenMEM) and the deepening of the range of courses in this area. He will take over from Joachim Veit as co-project manager of the academy project.
The Swiss Violin Making School Brienz Foundation honors violinist Meret Lüthi with a "Golden Bow".
PM/SMZ/wb
(translation: AI)
- Nov 06, 2023
Meret Lüthi (Image: Guillaume Perret)
Meret Lüthi studied in Bern with Monika Urbaniak-Lisik and Eva Zurbrügg and in Basel with Walter Levin. She continued her training on the baroque violin with Anton Steck in Trossingen. As a specialist in early music, she teaches baroque violin and historically informed performance practice at Bern University of the Arts. In 2017 she was awarded the Music Prize of the Canton of Bern and in 2020 the Culture Prize of the Bürgi-Willert Foundation.
The Brienz jury honored Meret Lüthi "for building up her internationally renowned ensemble Les Passions de l'Âme and for sharing her impressive wealth of ideas and captivating programs with the public for over 15 years". Previous recipients of a Golden Bow include Hans Heinz Schneeberger, Thomas and Patrick Demenga, Thomas Füri, Thomas Zehetmair, Tabea Zimmermann, Patricia Kopatchinskaja and Kim Kashkashian. The prize, a high-quality engraved bow from Finkel Bogenwerkstätte Brienz AG, is presented at the opening concert of the Meiringen Music Festival Week.
Konsibern continues to receive support from the city
The Municipal Council, the executive body of the City of Bern, has approved the service agreement with the Bern Conservatory Foundation for the year 2024.
PM/SMZ/wb
(translation: AI)
- Nov 02, 2023
(Image: Konsibern)Konsibern
The prerequisite for supporting the Bern Conservatory of Music (Konsibern) is that the voters of the City of Bern approve the 2024 budget on November 19, 2023. The budget also includes the funds for Konsibern. The music school's services are to be paid for with a sum of around four million francs for 2024. This includes additional costs of 166,504 francs, which are due to an increase in the number of lessons, an increase in teachers' salaries and higher rental costs.
The music school was founded in 1858 by the Bernese Music Society BMG. With the founding of the Bern University of the Arts HKB in 2000, the general music school department of the former conservatory was transformed into an independent institution and the Bern Conservatory Music School Foundation was established as a competence center for amateur music-making.
Pro Helvetia Director hands over divisional responsibility
Philippe Bischof is handing over responsibility for the External Network & International Affairs division to Deputy Director Jérôme Benoît with immediate effect. The reason is a private relationship.
PM/SMZ/wb
(translation: AI)
- Nov 01, 2023
Philippe Bischof (Image: Youtube video still)
According to the foundation's press release, the personnel and organizational changes are being made in connection with a private relationship that has arisen at management level. By handing over responsibility for the External Network & International Affairs division to Benoît, Bischof will no longer report directly to his partner with immediate effect. She herself is no longer a member of the Executive Board until the end of June 2025. In the course of developing the new management structure, Bischof also informed the Board of Trustees of his wish to end his mandate on June 30, 2025.
Pro Helvetia writes that the timing of the change of director at the end of June 2025 is justified in terms of content, as the financing and implementation of the new cultural message will be secured by this time and the business can be handed over accordingly. After his time at Pro Helvetia, Philippe Bischof would like to move on to the next stage of his career and have more time for his private life. The management position will be advertised in 2024.
Christoph Müller hands over management of the Gstaad Festival
Christoph Müller ends his engagement as Artistic Director of the Gstaad Menuhin Festival at the end of the three-year cycle "Wandel 2023 - 2025".
PM/SMZ/wb
(translation: AI)
- Oct 31, 2023
Christoph Müller (Image: Menhuin Festival/Adrian Moser)
Under the artistic direction of Christoph Müller, the festival has developed from a pure concert festival into a versatile and multi-faceted festival, according to the press release. This also includes talent promotion and mediation. In addition to the further development of concert operations, Müller has gradually built up the Gstaad Academy with its five academies, the Gstaad Festival Orchestra, the digital offerings as part of the Gstaad Digital Festival and numerous other projects since 2008. The flagship of the Gstaad Academy is the Gstaad Conducting Academy, launched in 2014, which also awards the annual Neeme Järvi Prize.
Christoph Müller studied cello in Bern and Zurich and was a cellist in the Basel Chamber Orchestra until 2013. He was managing director and orchestra director of the Basel Chamber Orchestra until 2010. He has been Artistic Director of the Menuhin Festival Gstaad since 2002. From 2005 to 2013 he was also Artistic Director of the Interlaken Music Festival (Interlaken Classiques).
St. Gallen Cultural Office with co-management
Sabina Brunnschweiler and Christopher Rühle will lead the Office for Culture of the Canton of St. Gallen in a co-management model from next spring.
PM/SMZ/wb
(translation: AI)
- Oct 30, 2023
Christopher Rühle and Sabina Brunnschweiler (Image: Canton of St. Gallen)
Christopher Rühle and Sabina Brunnschweiler succeed Tanja Scartazzini, who headed the Office of Culture until last August and is now working for the City of Winterthur. Rühle is already working in the office as Head of Legal Affairs and Head of the Cultural Heritage Department. Sabina Brunnschweiler currently works at the Canton of Zurich's Department of Culture as head of the promotion team.
The new heads of office will work together on overarching management tasks. However, responsibility for the individual areas of the office, which has around one hundred employees, will be divided up. According to current plans, Sabina Brunnschweiler will be responsible for cultural promotion, state archives and the cantonal library, while Christopher Rühle will be in charge of monument preservation, archaeology and cultural heritage.
Christopher Rühle, who holds a doctorate in political science, grew up in Wil, where he also lives. He has worked at the Office of Culture for 16 years, currently as Head of Legal Affairs and Head of the Cultural Heritage Department. He has completed project skills and further training in the areas of management, business administration and culture and is a long-standing member of the Office's management team and also a member of the current interim management team. Rühle is married and the father of a daughter and two sons.
Sabina Brunnschweiler grew up in Toggenburg. She studied German linguistics and literature, general history and journalism. She worked as a journalist in the canton of St.Gallen for several years and then moved to the Office for Culture for a few years, where she worked in the cultural promotion department. In 2011, she moved to the Canton of Zurich in the Culture Department. Since 2018, she has been a member of the management team and head of the funding team and the dance and theater department. She is married and the mother of two daughters.
Luginbühl becomes Chairman of the Board of Trustees of Bühnen Bern
Werner Luginbühl succeeds Nadine Borter as President of the Board of Trustees of Bühnen Bern. Above all, he must oversee the complete conversion of operations to a stagione model.
PM/SMZ/wb
(translation: AI)
- Oct 27, 2023
Werner Luginbühl (Image: zVg)
Luginbühl's predecessor Nadine Borter will continue to chair the board until the end of 2023. As President of the Board of Trustees, she has done important stabilization work, writes the city. Under her presidency, "talks with the trade unions were steered in a constructive direction, a code of conduct was drawn up, new appointments were made to the artistic directorate and all division heads, the coronavirus pandemic was dealt with and the institution was well positioned under the new name Bühnen Bern".
Following the allegations of abuse in the dance company, Nadine Borter ensured a comprehensive investigation, internal training and the development of prevention strategies. The Foundation Board responded to the reduced performance contract with less public funding by switching to stagione operation, thus ensuring that the three stage sections and the Bern Symphony Orchestra were maintained.
Werner Luginbühl headed the Canton of Bern's Department of Justice, Communes and Churches as a member of the cantonal government from 1998 to 2008. From 2007 to 2019, he represented the Canton of Berne in the Council of States and at the same time worked for Swiss Mobiliar as Head of Public Affairs. He has been Chairman of the Swiss Federal Electricity Commission (ElCom) since March 1, 2020. In recent years, Werner Luginbühl has chaired cultural institutions in various areas.
Cultural awards of the City of Zurich 2023
The City of Zurich honors 22 artists and three collectives. The award for special cultural merit goes to the cultural mediator, performer and musician Brandy Butler.
PM/SMZ/wb
(translation: AI)
- Oct 26, 2023
Alina Amuri (Image: Youtube video still)
In the Jazz, Rock, Pop category, Alina Amuri, Sibylla Giger and Belia Winnewisser will be awarded years of work (CHF 48,000 each). In the classical/new music category, the Ensemble Kiosk and Sebastian Hofmann & Martin Lorenz will receive the same amount of work years.
Brandy Butler has developed into one of the most important cultural mediators and activists in the city of Zurich in recent years, according to the city's press release. She is also "part of and the driving force behind various local and national initiatives". For example, she has been "organizing the highly acclaimed Drag Story Time" for years. She also organizes the Black Performance Lab, where queer people of colour (PoC) performers can reorient themselves. The award for special cultural merit is endowed with 20,000 francs.
Mayor Corine Mauch will present the awards totaling CHF 677,000 on Friday, November 24, 2023, at a ceremony for invited guests at Kaufleuten. The work years, work grants and awards are a key instrument of the City of Zurich for promoting the independent performing arts community.
Winner of the first Paul Juon chamber music competition
Ten ensembles were invited to take part in the first Paul Juon Chamber Music Competition at the Kunsthalle Appenzell. The winners were Ensemble Fokus, the Loewe Quartet and the Zeitgeist Trio.
PM/SMZ/wb
(translation: AI)
- Oct 25, 2023
Winners of the competition (Image: Förderkreis Kammermusik Schweiz)
The members of Ensemble Fokus, founded in 2022, come from all over Switzerland and Germany. They are Daniela Engel, Sarah-Maria Schmid, Pauline Zahno, Alexander Rauch and Adèle Bagein. The Loewe Quartet, an ensemble of students from the Hochschule für Musik in Zurich, unites Bastian Loewe, Livia Bechtold, Juan Carlos Escobar Ossa and Alina Isabel Morger. The Zeitgeist Trio was founded by Tim Crawford, Martin Egidi and Martin Jollet, students at the Hochschule für Musik Basel. The winner of the special Paul Juon prize donated by Myriam Gebert for the best interpretation of a work by Paul Juon is the Alas Quartet.
The Swiss Chamber Music Association is the supporting association and organizer of the Lake Constance Chamber Music Festival and, in collaboration with the Paul Juon Society, organizer of the Paul Juon Chamber Music Competition with concert placement. The newly founded Paul Juon Chamber Music Competition is aimed at young Swiss ensembles and offers the winning ensembles a three-year concert placement with substantial financial support for the concerts.
All winning ensembles not only receive prize money, but are also included in the concert program of the Swiss Chamber Music Association for three years. Concert organizers who engage winning ensembles for public concerts also receive financial support from the Förderkreis. At the same time, the Förderkreis Kammermusik Schweiz guarantees the musicians appropriate remuneration.
Revaz's choice attracts international attention
The election of cellist Estelle Revaz to the National Council has attracted international attention in the specialist press.
PM/SMZ/wb
(translation: AI)
- Oct 24, 2023
Estelle Revaz (Image: Nadège Gaillard)
Revaz successfully stood as a candidate for the Geneva SP. She previously made a name for herself during the pandemic with her commitment to coronavirus compensation. In the National Council, she wants to campaign for cultural policy issues. The Austrian-Swiss cellist performs regularly in Europe, Asia and South America and at the Gstaad Menuhin Festival, the Verbier Festival, the International Festival of Colmar and the Pablo Casals Festival.
Revaz's choice was reported in the Luxembourg trade magazine Pizzicato and the renowned British online magazine Slipped Disc, among others.
Change of management at Unit Records
The Swiss label Unit Records comes into new hands: bassists Andreas Waelti and Luca Sisera succeed Harald Haerter.
PM/SMZ/wb
(translation: AI)
- Oct 23, 2023
Andreas Waelti and Luca Sisera (Image: Andi Schnoz)
Founded in 1983 by Swiss jazz musicians Jürg Solothurnmann, Hans Kennel, Paul Haag and Urs Blöchlinger as a "platform for innovative musicians from the Swiss-German scene", the label was taken over in 1991 by Pius Knüsel, who later became director of the Swiss Arts Council Pro Helvetia. From 1996 to 2005, the renowned drummer Lucas Niggli managed Unit Records until guitarist Harald Haerter took over the reins in 2005.
After almost two decades, Harald Haerter is now handing over the reins to bassists Andreas Waelti and Luca Sisera. In recent years, both musicians have made a name for themselves as sidemen and bandleaders with a remarkably busy international concert schedule. Their artistic work has been documented in detail by numerous releases on various labels and they are well connected in the European scene.
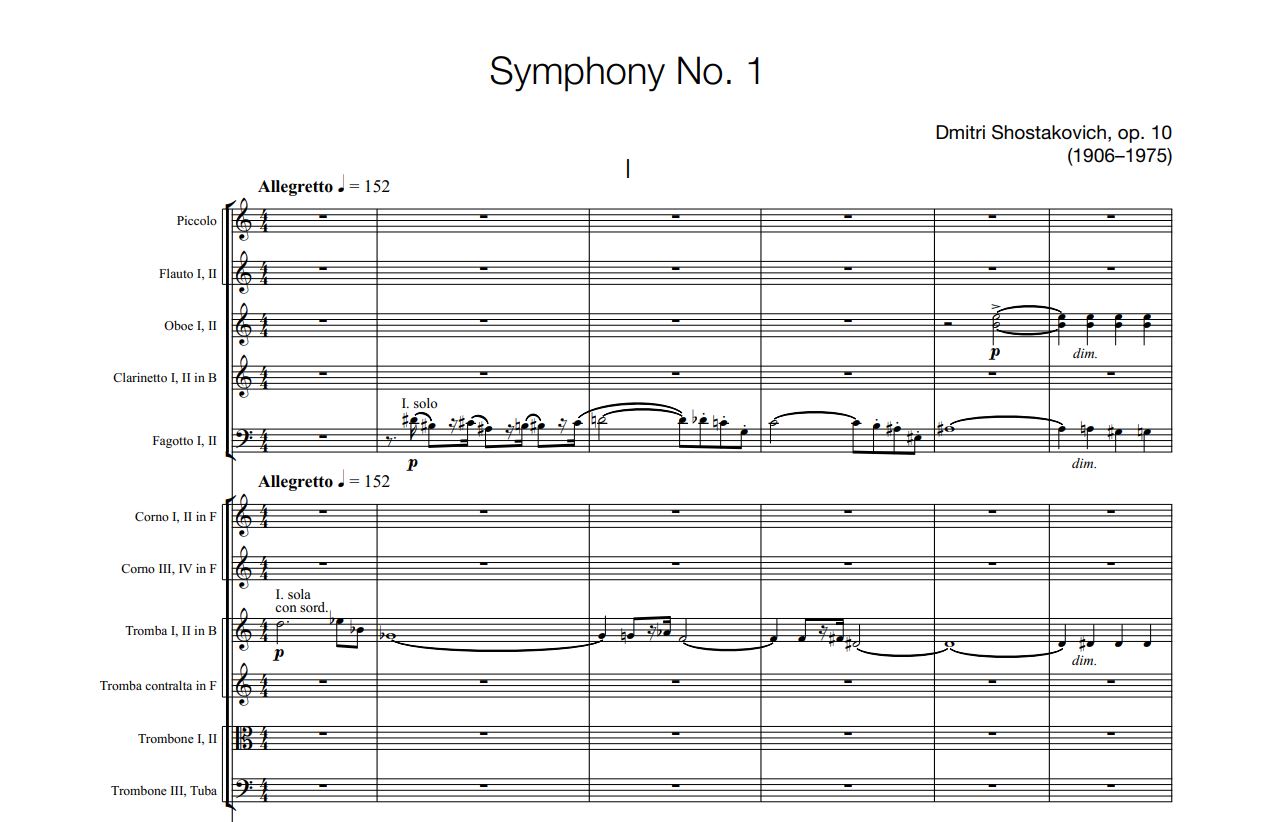
Shostakovich's symphonies in a new edition
The publishers Boosey & Hawkes and Sikorski are publishing a corrected new edition of all 15 symphonies by Dmitri Shostakovich.
PM/SMZ/wb
(translation: AI)
- Oct 20, 2023
(Image: Boosey & Hawkes)
Parts of the new, revised and corrected edition of all Shostakovich symphonies are now available. The first group of four publications spans the composer's life from his youthful Symphony No. 1 through Nos. 9 and 11 to his enigmatic farewell with No. 15.
No. 15 is to be completed by the 50th anniversary of the composer's death in 2025. The first four volumes of the edition, Nos. 1, 9, 11 and 15, are published as large-format study scores for optimum readability. All scores and the accompanying orchestral parts have been provided with new computer typesetting, and the orchestral parts are also compatible for performance with the scores in "The New Collected Works of Dmitri Shostakovich".
As the British music journalist Norman Lebrecht explains in his magazine Slipped Disk, the publishers do not specify how serious the errors were in earlier scores from the Soviet and post-Soviet era.